EUTHANASIA AND THE
RIGHT
TO DIE
So what is to be made of the 1990 merger between Concern
for Dying and the Society for the Right to Die, the media attention given
to Jack
Kevorkian's
suicide machine, and Derek Humphry's Final Exit reaching the top
of the New York Times best-seller list in 1991 (and its video version appearing
on Oregon television and in Amazon.com's
inventory in 2000)? Have we reached the point
where dying has become another form of consumer resistance? Certainly one common theme underlying these developments is the failure of the contemporary
death ritual for both the dying and the bereaved.
|
SYMBOLS OF THE EUTHANASIA DEBATE

Though most euthanasia cases involve the
elderly, it is interesting to note how often the right-to-die campaign
has been dramatized in the cases of brain-damaged young women: Karen
Ann Quinlan (1975-1985), Nancy
Cruzan (1983-1990), and Terri
Schiavo (1990- ).
|
The loss of control experienced by institutionalized
terminally ill patients is a central motif of much thanatological research.
Dying patients' basic human rights are seen to be violated when they lack
the knowledge and power to make decisions which, in turn, diminishes dignity.
Patients have the right to know their condition, to choose or to reject
the treatment regimen, to choose or to reject attempts to prolong their
life, and to decide fully as to the disposal of their remains. They also
have the right to ritually vent their fears and frustrations. (Consider
the findings of David Spiegel, whose study of women with metastic breast
cancer found that those who belonged to a psychotherapy group survived
almost twice as long on average as those who did not participate in a support
group, and reported less depression, anxiety and pain.) For the moving story of
John Graham's death check out Soundprint's
"A
Matter of Life and Death: Assisted Suicide in Australia" (Michael
Lutsky, producer).
As is the case with any ending--whether it be music resolutions, the denouements of
literature and drama, conclusion sections of research papers, the logic of desserts, or the
completion of a human life--failure to culminate "correctly" jeopardizes the overall
meaningfulness of the social product. Endings occasion special insight.
Representing consummation and closure, endings reveal the connections between
means and goals. They demand summations of the worthiness, coherence, and
meaningfulness of their encounters with time. Further, the endings of role
careers and lives can be the most individualizing of experiences: Individuals
"in exit" no longer need to conform to trivialities of mass culture
nor to the norms of the status hierarchy; one can say what one likes for
there is nothing to lose. For these reasons, endings are highly
ritualized.
From this perspective, the problem of our times is
the apparent lack of cultural consensus over exactly how endings --whether
from work, the family, or from life itself-- should be ideally conducted.
It is for this reason that we now witness expanding political and legal
involvements in status terminations. In 1997, the
U.S. Supreme Court will decide if states can prosecute physicians for assisting
in the suicides of their competent, terminally ill patients. We do
know that "good" endings require personal control and the minimization
of degradation. As a consequence, we're witnessing the emergence of the
death awareness movement that features the right-to-die, euthanasia, and
hospice movements as well as the public's receptivity to K�bler-Ross's
stages of the death process. This, in turn, is regenerating a life awareness
movement. As Martin Luther King said on the eve of his assassination, no
one is truly free to live until one is free to die.
Click here to see

Given the results of an eight-year clinical study of dying in
America, (Study
to Understand Prognoses and Preferences for Outcomes and Risks of Treatments,
funded by the Robert Wood Johnson Foundation; William Knaus and Joanne
Lynn principal investigators), revealing that one-half of conscious patients who died in hospitals
reported moderate to severe pain at least one-half of the time, and given the survey results of
1,400 doctors and nurses at five major hospitals in different parts of the country (published in
the January 1993 issue of the American Journal of Public Health) indicating that
81% agreed that "the most common form of narcotic abuse in caring for dying patients is
undertreatment of pain" with nearly half of the attending physicians and nurses and 70% of
resident physicians reporting having acted against their conscience by not aggressively
treating
terminally ill patients, perhaps we would not be faced with the euthanasia debate if adequate
pain control had been administered. Check out the philosophy and resources at the
Palliative Page.
GENERAL
REFERENCES
LEGAL RULINGS,
BRIEFS, AND ISSUES
- Ninth
Circuit Court of Appeals Decision of March, 1996
- Second
Circuit Court of Appeals Decision of April, 1996: Quill v. Vacco
-
Rights
of the Terminally Ill in Australia, 1995

PROPONENTS
- Right to Die Society
of Canada--"Advancing the Art & Science of
Dying Well"
- FinalExit.org's Euthanasia World Directory
- Hemlock Society USA
-
Yahoo's Euthanasia Listings: Proponents
- Views
of late Noel Earley, victim of ALS
- Robert
Neils's (President of Dying Well Network) book "Death with Dignity FAQs"
- World Federation of
Right to Die Societies' website
(and a listing of members here)
- EXIT (formerly Voluntary
Euthanasia Society of Scotland)
- Dying
with Dignity (Canadian Society)
- Voluntary
Euthanasia Society (UK and Wales) --with daily international news items and
a searchable news database
- The Voluntary Euthanasia Society of New Zealand
- Euthanasia
in the Netherlands
- LAST
RIGHTS Electronic Journal
ADVERSARIES
-
Yahoo's Euthanasia Listings: Opposing Views
- International Anti-Euthanasia Task
Force
- Citizens United Resisting Euthanasia
(CURE, Ltd.): "Practicing Compassion, Unity, Research, and Education"
- Euthanasia
(links from Ohio Right to Life)
-
Ezekiel Emanuel's "Whose Right to Die?" from The Atlantic Monthly
- Ted Gerk's "The
Kevorkian Papers"
- Not Dead Yet! Disabled activists
speak their opposition
PHYSICIAN-ASSISTED SUICIDE
There is a fine moral line between euthanasia and physician-assisted suicide.
Physicians still, however, control the final passage as terminally ill patients'
ability to have legal access to lethal drugs is contingent on doctors'
approval. In the July 2000 edition of Reason magazine, Thomas Szasz
speaks of "the galloping therapeutic state, where
increasingly we are giving away our existential choices and responsibilities to
doctors." He notes that if one buys a rope to hang oneself we don't
refer to it as "merchant- assisted suicide." And is accelerating
the inevitable really "suicide"?
- Thomas A. Bowden's "Assisted Suicide: A Moral Right" produced by the
Ayn Rand Institute's MediaLink
KEVORKIAN'S BOX
SCORE
At the center of this moral hurricane is Dr. Jack Kevorkian,
a Michigan pathologist (whose business card reads "Jack Kevorkian,
M.D. Bioethics and Obitiatry. Special Death Counseling") who created
suicide machines to allow terminally ill patients to kill themselves in
supposedly humane and painless ways. In his 1991 book Prescription:
Medicine--The Goodness of Planned Death, he speaks of the "Stone-Age
ethics of space-age medicine" and of his personal crusade for physician-
assisted suicide. His highly publicized activities have been viewed by
others in a multitude of ways, from his being a godsend to a serial
killer.

Kevorkian is not alone is his acceleration of the death
process of the terminally ill. A
1996 study by David A. Asch of over 800 critical-care nurses, for instance,
revealed nearly one in five admitting to hastening the deaths of terminally
ill patients--16 percent by performing euthanasia or assisting in suicide,
and another 4 percent by only pretending to live life- sustaining treatment
ordered by physicians.
- Patients
helped to die by Dr. Jack Kevorkian
THOUGHTS ON THE
"SLIPPERY
SLOPE"
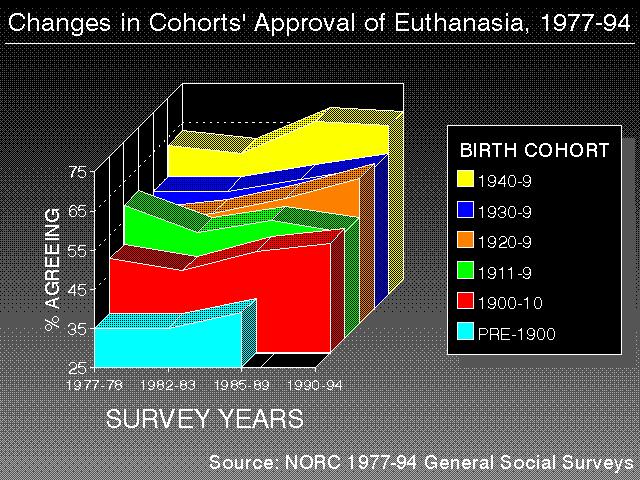
To what extent do Americans' orientations toward abortion,
euthanasia, and the moral right of the terminally ill to take their own
lives "hang together" in their minds? Does increasing social
approval of one--say, approval of physician-assisted suicide--lead over
time to increasing social approval of the others?
Increasingly public discourse features debates over
semantics and either the blurring or sharpening of distinctions. For instance,
in the case of euthanasia there is the distinction between mercy killing
and the merciful use of drugs that, like the "morphine drip,"
may "unintentionally" hasten the death of a terminally-ill individual.
At a public lecture at Trinity University (October 13, 1995), Ralph Miro
argued that the difference between a pain-plagued terminally ill patient
taking a legally prescribed lethal dose of pharmaceuticals and the suicide
of one depressed is analogous to the difference between love-making and
rape.
On the other hand, proponents of the slippery-slope
thesis claim that such blurrings or new distinctions lead to ever-widening
acceptances of death. Once terminal patients in pain are allowed to die,
then does it not become harder to deny the same right to someone in terrible
pain who faces not death but rather a life of torment? Further, if competent
individuals are allowed to seek death, then does it not become harder to
deny terminating the lives of sick infants or adults in comas? At some
point, so the argument goes, we move from assisted suicide to homicide
and then to genocide, the ultimate moral abyss.
In her 1994 ruling striking down a 140-year-old
Washington
State ban on assisted suicide, Judge Barbara Rothstein of U.S. District
Court in Seattle said
The suffering of a terminally ill person cannot be deemed any less intimate
or personal, or any less deserving of protection from unwarranted governmental
interference than that of a pregnant woman. ... Like the abortion decision,
the decision of a terminally ill person to end his or her life `involves
the most intimate and personal choices a person can make in a lifetime,'
and constitutes a `choice central to personal dignity and
autonomy.'
Let's begin by examining longitudinal trends in Americans'
responses to the following three questions (recognizing
the sensitivity of responses to question wording):
- Do you think it should be possible for a pregnant
woman to obtain a legal abortion if the woman wants it for any reason?
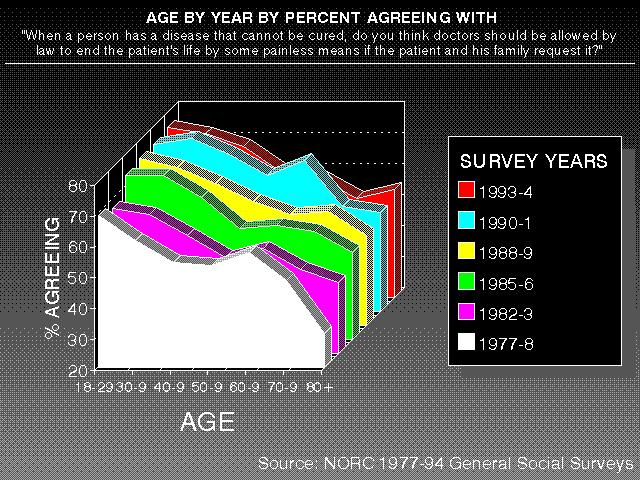
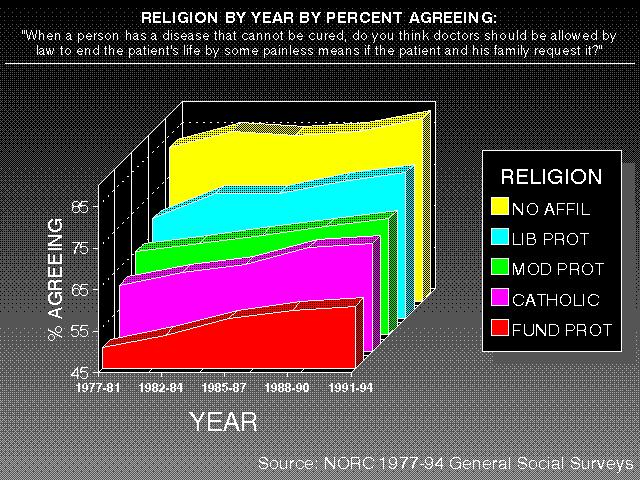
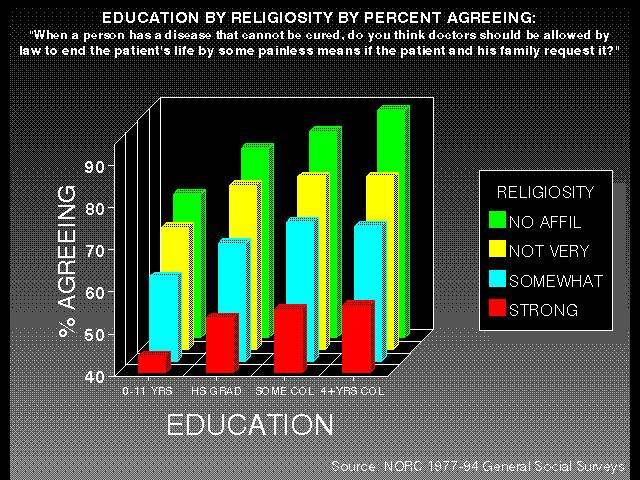
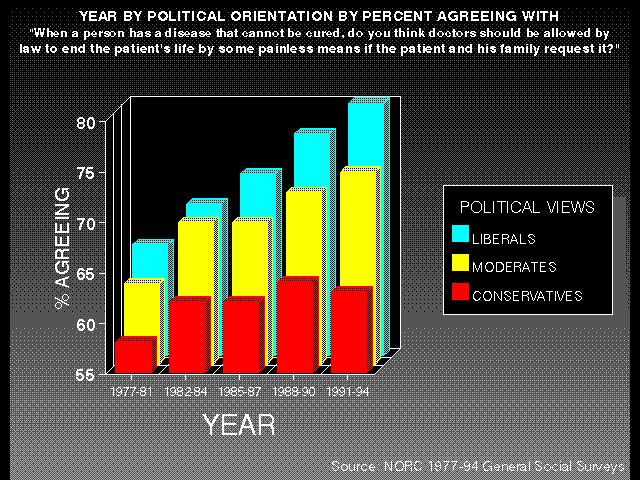
- When a person has a disease that cannot be cured,
do you think doctors should be allowed by law to end the patient's life
by some painless means if the patient and his family request it?
- Do you think a person has the right to end his or
her own life if this person has an incurable disease?
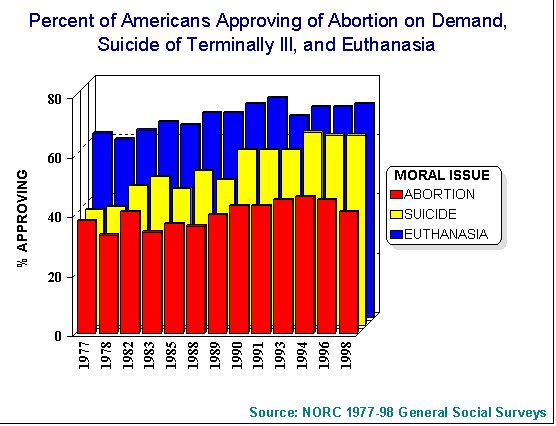
Combining responses from the NORC General Social
Surveys
between the years 1977 and 1998 (n=19,000+), we find Americans are more
likely to approve of euthanasia (68%) than suicide (53%) or abortion on
demand (40%). Click here to see Annual rates of
approval of euthanasia, suicide and abortion. As can be seen in this
figure, the moral issue with the greatest change in approval was suicide
of the terminally ill, which Americans were nearly two-thirds more likely
to approve of in 1998 (64%) than in 1977 (38%).
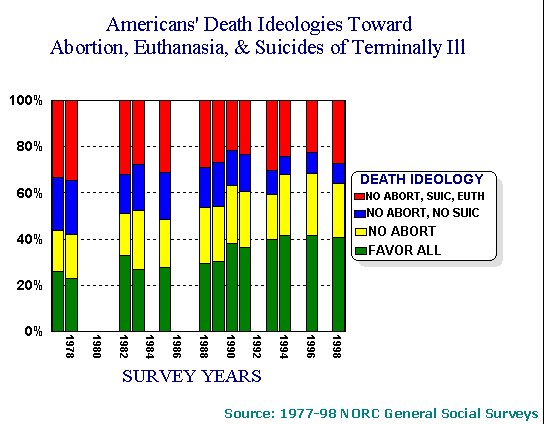
The number of Americans approving all three of
these ways of ending life increased from 26% in 1977 to 38% in 1998, while
the number disapproving of all declined from 33% to 26%. Click here to
see Annual rates of number of approvals of euthanasia,
suicide and abortion.
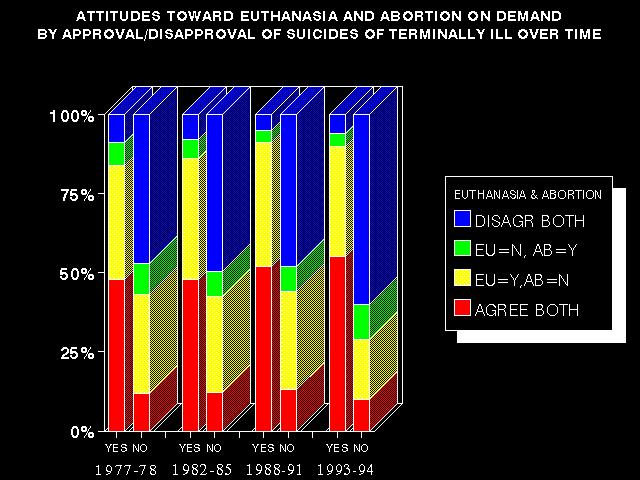
Since the greatest change was in approval of the moral
right of the terminally ill to commit suicide, let's examine the relationship
between attitudes toward euthanasia and abortion among those who do and
do not approve of suicide and how this has changed over time. Click here
to see The relationship between attitudes toward
euthanasia and abortion by approval/disapproval of suicide. Several
trends are worth noting:
- Among those approving of the right to commit suicide,
the percentage approving of both abortion and euthanasia increased from 52 to 55 percent.
- Among those disapproving of the right to commit suicide,
the percentage disapproving of both abortion and euthanasia increased from 45 to
62 percent.
- While in the 1977-78 period those approving of suicide
were four times more likely to approve of both euthanasia and abortion
than those disapproving of suicide, by 1998 there was nearly a five-fold
difference.
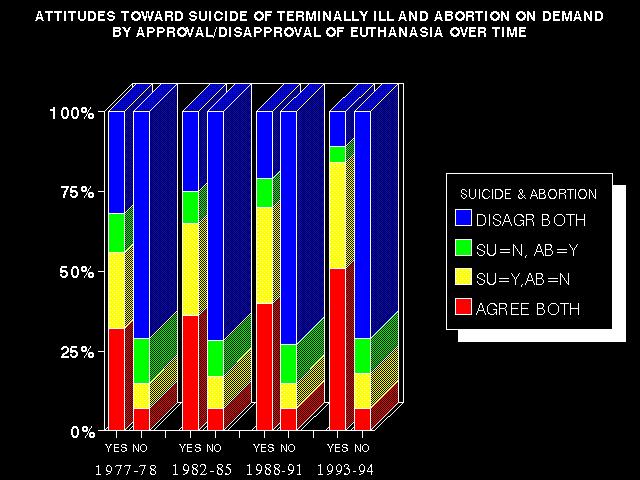
Now let's examine the relationship between attitudes
toward suicide and abortion among those who do and do not approve of euthanasia
and how this has changed over time. Click here to see The
relationship between attitudes toward suicide and abortion by approval/disapproval
of euthanasia. Several trends are worth noting:
- Among those approving of euthanasia, the percentage
of Americans approving of both abortion and suicide increased dramatically,
from 32 to 51 percent. For this group, the percentage disapproving of both
abortion and suicide declined by nearly two-thirds, from 32 to 11 percent.
- Among those disapproving of euthanasia, there was
virtually no change in the relationship between attitudes toward abortion.
- While in the 1977-78 period those approving of euthanasia
were 4.6 times more likely to approve of both euthanasia and abortion than
those disapproving of euthanasia, by 1993-94 euthanasia supporters were
7.3 times more likely to approve of both euthanasia and abortion than the
non-supporters.
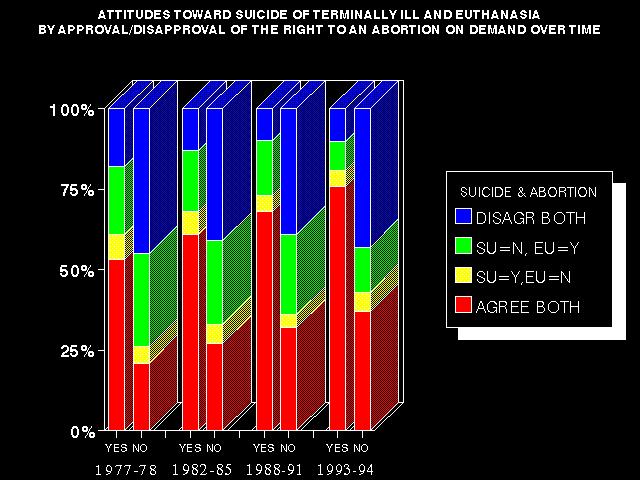
Finally, let's consider the relationship between attitudes
toward suicide and euthanasia among those who do and do not approve the
right of a pregnant woman to have an abortion and how this has changed
over time. Click here to see The relationship between
attitudes toward suicide and abortion by approval/disapproval of euthanasia.
Trends:
- Among those approving of abortion, the percentage
of Americans approving of both suicide and euthanasia increased from 53
to 75 percent.
- Among those disapproving of abortion, the percent
approving of both euthanasia and suicide increased 21 to 37 percent. Of these
folks, the percent disapproving of both euthanasia and suicide remained
virtually constant.
- For both those approving and disapproving of abortion,
the percent of those approving only of either euthanasia or suicide but
not both declined significantly.
Bottom line: there is a great moral polarization in
American society on matters of euthanasia, suicide of the terminally ill,
and abortion, and it is increasing over time. Further, as these death attitudes
coalesce into polarized ideologies they are also becoming increasing correlated
with individuals' positions within the status hierarchy (within social
classes).
What does this polarization mean? There is emerging
two ideological cores, each with its own rhetoric and each spawning (because
of the existence of the other) its own extreme fringe elements. It is probably
not the case that ideology leads to these social movements, but rather
these movements are emerging in collective opposition to each other. Ideological
themes emerge only later, as justifications for the movements'
actions.
Core 1 is comprised of the "pro-life" folks:
moral absolutists (who see the moral issues in black-and-white terms instead
of shades of gray), politically conservative, religious fundamentalists
(the Christian Coalition is out to legislate religious views), anti- euthanasia,
pro-capital punishment, favoring the right to bear arms (Second Amendment
Activists), anti-government (believing government should stay out of people's
private lives), pro-business, anti-environmentalist, and favoring a strong
military. Allying themselves with this emerging core are Christian home-schoolers
and conspiracy theorists. These are the people who belief that the killing
of abortionists is morally justified; it is not murder to murder a murderer.
The extreme fringe of this core has found a voice in the millennial movements,
like Christian Patriots and state militias (i.e., the Militia of Montana,
who claimed that the UN plan to partition the United States into 9 zones
appeared in 1994 on the back of Kix cereal boxes).
Core 2 is comprised of the "pro-choice"
folks. They are moral relativists (who see many shades of moral grays);
politically liberal, favoring gay rights, abortion rights, and right-to-
die legislation; secular humanists; environmentalists; and favoring a scaled
down military.
THE INTERRELATIONSHIPS
BETWEEN AMERICANS'
ATTITUDES TOWARD EUTHANASIA AND THE LEGALIZATION OF
MARIJUANA
Have you noticed how debates over "good deaths" have put
marijuana back in the news recently? And you thought the drug was basically
safely locked away back in the sixties and seventies.
Percent approving of legalization of marijuana by responses
to "When a person has a disease that cannot be cured, do you think
doctors should be allowed by law to end the patient's life by some painless
means if the patient and his family request it?"
|
1978 |
1983 |
1986 |
1988 |
1989 |
1990 |
1991 |
1993 |
1994 |
1996 |
1998 |
|
YES
|
39% |
25% |
23% |
22% |
18% |
20% |
21% |
28% |
28% |
33% |
36% |
| NO |
18 |
13 |
10 |
9 |
7 |
9 |
9 |
14 |
11 |
12 |
13 |
% SHOULD
LEGALIZE |
30 |
21 |
18 |
18 |
17 |
17 |
19 |
23 |
24 |
27 |
29 |
% EUTHAN
=YES |
60 |
66 |
68 |
69 |
69 |
72 |
74 |
68 |
71 |
71 |
72 |
Looking at the YES and NO rows of the above table within the 1978
column we see how, for instance, of those supporting physician-assisted
death in 1978, 39% approved of the legalization of marijuana, compared
with only 18% of those opposing physician-assisted death. In that year
30% of Americans in total approved of the drug's legalization and 60% approved
of euthanasia.

 Return
to Kearl's Death Index
Return
to Kearl's Death Index
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}